Entry Version:
Citation:
Pancreapedia: Exocrine Pancreas Knowledge Base, DOI: 10.3998/panc.2015.33
| Attachment | Size |
|---|---|
| 368.91 KB |
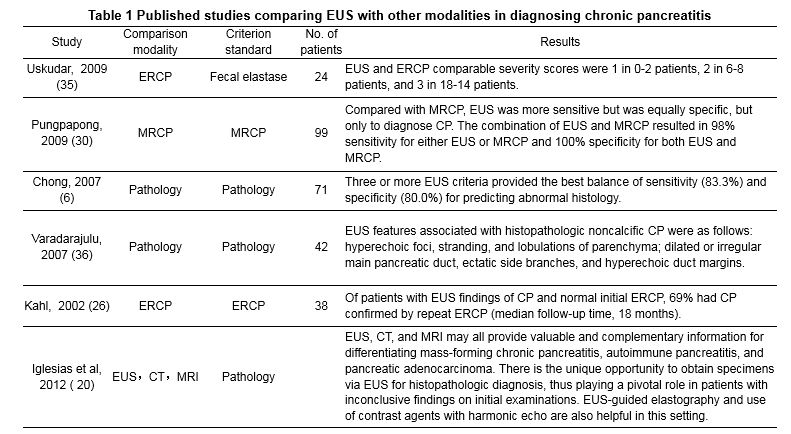
Chronic pancreatitis (CP) is a consequence of various disorders—largely chronic alcoholism, biliary diseases, and trauma—and is signaled by specific risk factors, known signs and symptoms, and distinct abnormalities of imaging and laboratory diagnostics. Pancreatic calcification and dilatation of the pancreatic duct are characteristics findings of CP on noninvasive imaging studies, such as computed tomography (CT) and magnetic resonance imaging (MRI) (14). Although the latter are considered modalities of choice, endoscopic ultrasound (EUS) is now also viewed as one of the most sensitive methods for detecting pancreatic lesions, given the close proximity of the transducer to the pancreas (4, 21, 27, 28). Since 1986, there have been numerous studies reporting the use of endoscopic ultrasound for the diagnosis of chronic pancreatitis. EUS has been amply compared with noninvasive cross-sectional imaging and endoscopic retrograde cholangiopancreatography (ERCP) (6, 20, 26, 30, 33, 35, 36) in terms of accuracy in diagnosing CP (as shown in Table 1). The utility of EUS stems from its capacity to demonstrate subtle alterations in pancreatic structure that escape traditional imaging and laboratory tests of pancreatic function. The sensitivity of EUS may be further heightened by limiting the core criteria required to diagnose CP.
In EUS studies of the pancreas, non-homogenous changes of parenchyma, particularly hyperechoic foci or strands, lobulation, calcifications, and cysts, and ductal alterations, including a hyperechoic wall, dilatation and/or tortuosity of the main duct, intraductal hyperechoic foci, and ectatic side branches are grounds for a diagnosis of CP (4, 21, 27, 28). The severity of CP (mild, moderate, severe) may also be gauged accordingly (21), although standardized diagnostic guidelines have yet to be adopted.
The most frequently used classification was described by Wiersema et al. in 1993. There were 9 pancreatic criteria: hyperechoic foci, hyperechoic strands, lobularity, cyst, calcification, main pancreatic duct dilatation, side branch dilatation, pancreatic duct irregularity and hyperechoic duct margins (38). In April 2007, a new classification was proposed as part of an international consensus meeting in Rosemont, Illinois. The new criteria gave a different value, establishing major and minor criteria depending on the features found (5, 29). The Rosemont major criteria are: hyperecoic foci with shadowing and main pancreatic duct calculi (Major A) and lobularity with honeycombing (Major B). Minor criteria included cysts, dilated ducts ≥ 3.5 mm, irregular pancreatic duct contour, dilated side branches ≥ 1 mm, hyperechoic duct wall, strands, nonshadowing hyperechoic foci, and lobularity with noncontiguous lobules.These criteria are used to define 4 groups of patients normal pancreas, indeterminate, suggestive and consistent with CP (5). EUS diagnosis of CP on the basis of Rosemont criteria is shown in Table 2. In the study of Jimeno-Ayllón et al (24), they used Wiersema criteria and Rosemont classification in diagnosis of CP. The conclusion is: the new classification would be useful in patients with high suspicion of chronic pancreatitis with < 4 standard criteria but with more significance such as parenchymal lithiasis, lobularity or ductal calcifications.
EUS provides high-resolution imaging of the entire pancreas, enabling detailed parenchymal and ductal assessment. Normally, the parenchyma is homogeneous, with a finely reticular pattern, and the main duct has a smooth wall that is not dilated or hyperechoic. As a rule, the diameter of pancreatic duct is < 3 mm in at the head, < 2 mm at the neck, and < 1 mm at the tail; and side branches are not visible (21, 28). Allowing for anatomic variants that do occur, ventral pancreas may be more hypoechoic and heterogeneous than dorsal pancreas (Figure 1-3).
Determining whether hypoechoic and cystic lesions are inflammatory or neoplastic is still difficult (23) via conventional B-mode EUS imaging, but interpretation is aided significantly by fine needle aspiration (FNA) (1). Pancreatic neoplasms may coexist as complications of chronic pancreatitis (2), and cysts or inflammation may result from neoplastic obstruction of pancreatic duct.
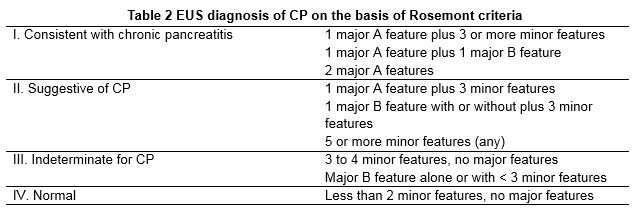

Figure 1. Chronic pancreatitis (Case 1). A 45-year-old male presented with chronic pancreatitis for 5 years. EUS showed heterogeneous echo pattern in the body (A) and neck (B) of pancreas: hyperechoic foci (dots); hyperechoic strands (linear); lobulation (pancreatic parenchyma is lobulated by linear hyperechos); irregular hypoechoic areas. Multiple FNA results were negative (with no signs of malignancy).

Figure 2. Chronic pancreatitis (Case 2). A 37-year-old male presented with cholecystolithiasis and recurrent pancreatitis for 5 years. (A) Radial EUS showed that the main pancreatic duct in the neck of pancreas was dilated (6mm). (B) EUS showed that the main pancreatic duct in the head of pancreas was dilated, while the main pancreatic duct near the ampulla wasn’t dilated. No tumor was found in the pancreatic head, and with combination of other clinical data, this lesion was finally diagnosed as chronic pancreatitis.

Figure 3. Chronic pancreatitis (Case 3). A 42-year- old male presented with cholecystolithiasis and chronic pancreatitis for 3 years. EUS showed that the parenchyma was displayed as heterogeneous, hyperechoic change in the head (A) and body (B) of pancreas, representing fibrosis.
In this context, the accuracy of EUS-guided FNA is quite high, demonstrating a sensitivity of 80-85% and a specificity near 100% (10, 34). However, this technique is technically demanding, often necessitating multiple passes to obtain tissue sufficient for a diagnosis (3, 11).
Furthermore, cytohistologic preparations may be falsely negative (despite repeated samplings), especially in patients with advanced chronic pancreatitis who develop solid masses (37).
Differentiating ductal adenocarcinoma from mass lesions of pancreatitis may be improved by spectral Doppler analysis, owing to the curious absence of venules in adenocarcinomas (arterioles only seen). Venules typically are not a prominent component of tumors, possibly due to the accompanying desmoplasia. On the other hand, both arterioles and venules of inflammatory lesions are usually detectable by Doppler (17, 32).
New techniques also have emerged to address this issue, namely contrast-enhanced EUS (CE-EUS) and EUS elastography (3, 31). CE-EUS is a novel approach where the usual high-resolution of ultrasound is intensified by contrast agents (8). CE-EUS may help to recognize and delineate necrotizing foci of acute pancreatitis, which ordinarily are not enhanced at a very early stage (31). The lack of nephrotoxicity shown by these agents is of particular importance, because most patients who are severely ill with pancreatitis also develop renal failure. In such instances, CT contrast enhancement is contraindicated. Interestingly, uptake of contrast focally in pancreatitis (7) or diffusely in autoimmune pancreatitis (16) is often similar to or better than that of normal pancreatic parenchyma. This feature may be useful in differentiating ductal adenocarcinoma.
Elastography is a method for assessing tissue rigidity in real time. Currently, elastographic evaluations of the gastrointestinal tract are done in conjunction with conventional EUS. The EUS probe is equipped with a processor and software that generate real-time elastographic data. Unlike first-generation technology, which is limited to qualitative estimates, today’s second generation tools allow quantitative analysis of tissue rigidity (9, 12, 13, 15, 19, 22, 25).
In qualitative elastography, compression-induced structural deformation is quantified in B-mode images, using the degree of deformation as an index of tissue rigidity (12, 13). As shown by Iglesias-Garcia et al (20), qualitative elastography of patients with CP proved to be irregularly colored, exhibiting green areas with predominantly blue heterogeneous strands. Analogous findings clearly differed in control subjects (with no pancreatic disease), where predominantly green and yellow homogeneous patterns were observed.
For quantitative elastography, there are two alternatives: the hue histogram and the calculated strain ratio. A hue histogram is a graphic representation of color distribution (hues) in a selected image field and is derived from qualitative EUS elastography data for a manually selected ROI within a standard elastographic image. The calculated strain ratio attempts to offset the comparative nature of qualitative elastographic patterns by analyzing the elastographic image of a target lesion relative to surrounding tissues (15, 18, 19, 22). Similar to a hue histogram, the strain ratio is calculated from standard qualitative EUS elastographic data, selecting two differing areas (A and B) for quantitative analysis. Area A encompasses as much of the target lesion as possible, excluding adjacent tissues, whereas area B is from a soft (red) reference area extraneous to the target lesion and preferably in the gut wall. The strain ratio is the quotient of B/A (19). Strain ratios of Rosemont categories are marked by significant statistical differences as follows: 1.80 (95% CI: 1.73-1.80), normal pancreas; 2.40 (95% CI: 2.21-2.56), indeterminate of CP; 2.85 (95% CI: 2.69-3.02), suggestive of CP; and 3.62 (95%CI: 3.24-3.99), consistent with CP (P<0.001) (Figure 4). In the study by Dominguez-Muñoz’ et al (9), strain ratio was used to predict pancreatic exocrine insufficiency (PEI) in patients with chronic pancreatitis. The conclusion was the degree of pancreatic fibrosis as measured by EUS-guided elastography allows quantification of the probability of PEI in patients with CP.
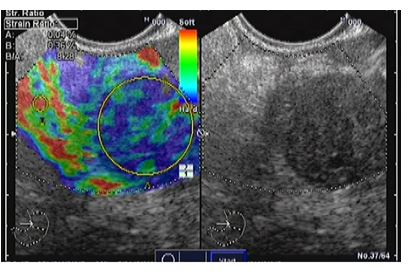
Figure 4. Quantitative EUS elastography based on strain ratio analysis of a solid pancreatic mass (pancreatic adenocarcinoma). We selected area A to represent pancreatic parenchyma, and area B to correspond to a soft area from the gut wall. The B/A ratio is displayed at the bottom of the image.
References
- Ardengh JC, Lopes CV, Campos AD, Pereira de Lima LF, Venco F, Módena JL. Endoscopic ultrasound and fine needle aspiration in chronic pancreatitis: differential diagnosis between pseudotumoral masses and pancreatic cancer. JOP 8(4):413-421, 2007. PMID: 17625292.
- Barthet M, Portal I, Boujaoude J, Bernard JP, Sahel J. Endoscopic ultrasonographic diagnosis of pancreatic cancer complicating chronic pancreatitis. Endoscopy 28(6):487-491, 1996. PMID: 8886634.
- Binmoeller KF, Rathod VD. Difficult pancreatic mass FNA: tips for success. Gastrointest Endosc 2002; 56:S86-S93, 2002. PMID: 12297756.
- Catalano MF. Diagnosing early-stage chronic pancreatitis: is endoscopic ultrasound a reliable modality? J Gastroenterol 42 Suppl 17: 78-84, 2007. PMID: 17238033.
- Catalano MF, Sahai A, Levy M, et al. EUS-based criteria for the diagnosis of chronic pancreatitis: the Rosemont classification. Gastrointest Endosc 69(7):1251-1261, 2009. PMID: 19243769.
- Chong AK, Hawes RH, Hoffman BJ, et al. Diagnostic performance of EUS for chronic pancreatitis: a comparison with histopathology. Gastrointest Endosc 65:808-814, 2007. PMID: 17466199.
- D’Onofrio M, Zamboni G, Tognolini A, et al. Mass-forming pancreatitis: value of contrast-enhanced ultrasonography. World J Gastroenterol 12: 4181-4184, 2006. PMID: 16830370.
- Dietrich CF, Ignee A, Frey H. Contrast-enhanced endoscopic ultrasound with low mechanical index: a new technique. Z Gastroenterol 43: 1219-1223, 2005. PMID: 16267707,
- Dominguez-Muñoz JE, Iglesias-Garcia J, Castiñeira Alvariño M, Luaces Regueira M, Lariño-Noia J. EUS elastography to predict pancreatic exocrine insufficiency in patients with chronic pancreatitis. Gastrointest Endosc 81(1):136-142, 2015. PMID: 25088920.
- Dumonceau JM, Polkowski M, Larghi A, et al. Indications, results, and clinical impact of endoscopic ultrasound (EUS)-guided sampling in gastroenterology: European Society of Gastrointestinal Endoscopy (ESGE) Clinical Guideline. Endoscopy 43:897-912, 2011. PMID: 21842456.
- Erickson RA, Sayage-Rabie L, Beisner RS. Factors’ predicting the number of EUS-guided fine-needle passes for diagnosis of pancreatic malignancies. Gastrointest Endosc 51:184-190, 2000. PMID: 10650262.
- Giovannini M. Contrast-enhanced endoscopic ultrasound and elastosonoendoscopy. Best Prac Res Clin Gastroenterol 23:767- 779, 2009. PMID: 19744639.
- Giovannini M. Endoscopic Ultrasound Elastography. Pancreatology 11:34-39, 2011. PMID: 21464585.
- Gleeson FC, Topazian M. Endoscopic retrograde cholangiopancreatography and endoscopic ultrasound for diagnosis of chronic pancreatitis. Curr Gastroenterol Rep 9:123-129, 2007. PMID: 17418057.
- Hirooka Y, Itoh A, Kawashima H, et al. Diagnosis of pancreatic disorders using contrast-enhanced endoscopic ultrasonography and endoscopic elastography. Clin Gastroenterol Hepatol 7:S63-S67, 2009. PMID: 19896102.
- Hocke M, Ignee A, Dietrich CF. Contrast-enhanced endoscopic ultrasound in the diagnosis of autoimmune pancreatitis. Endoscopy 43: 163-165, 2011. PMID: 21165827.
- Hocke M, Schulze E, Gottschalk P, et al. Contrast-enhanced endoscopic ultrasound in discrimination between focal pancreatitis and pancreatic cancer. World J Gastroenterol 12: 246-250, 2006. PMID: 16482625.
- Iglesias-Garcia J, Domínguez-Muñoz JE, Castiñeira-Alvariño M, Luaces-Regueira M, Lariño-Noia J. Quantitative elastography associated with endoscopic ultrasound for the diagnosis of chronic pancreatitis. Endoscopy 45(10):781-788, 2013. PMID: 24019131.
- Iglesias-Garcia J, Lariño-Noia J, Abdulkader I, et al. Quantitative endoscopic ultrasound elastography: an accurate method for the differentiation of solid pancreatic masses. Gastroenterology 139:1172-1180, 2010. PMID: 20600020.
- Iglesias-Garcia J, Lindkvist B, Lariño-Noia J, Domínguez-Muñoz JE. Endoscopic ultrasound elastography. Endosc Ultrasound 1(1): 8-16, 2012. PMID: 24949330.
- Iglesias-García J, Lindkvist B, Lariño-Noia J, Domínguez-Muñoz JE. The role of EUS in relation to other imaging modalities in the differential diagnosis between mass forming chronic pancreatitis, autoimmune pancreatitis and ductal pancreatic adenocarcinoma. Rev Esp Enferm Dig 104(6):315-321, 2012. PMID: 22738702.
- Irisawa A, Katakura K, Ohira H, Sato A, Bhutani MS, Hernandez LV, et al. Usefulness of endoscopic ultrasound to diagnose the severity of chronic pancreatitis. J Gastroenterol 42 Suppl 17:90-94, 2007. PMID: 17238035.
- Itoh Y, Itoh A, Kawashima H, Ohno E, Nakamura Y, Hiramatsu T, et al. Quantitative analysis of diagnosing pancreatic fibrosis using EUS-elastography (comparison with surgical specimens). J Gastroenterol 49(7):1183-92, 2014. PMID: 24026103.
- Jenssen C, Dietrich CF. Endoscopic ultrasound in chronic pancreatitis. Z Gastroenterol. 43(8):737-749, 2005. PMID: 16088771.
- Jimeno-Ayllón C, Pérez-García JI, Gómez-Ruiz CJ, García-Cano-Lizcano J, Morillas-Ariño J, Martínez-Fernández R, et al. Standard criteria versus Rosemont classification for EUS-diagnosis of chronic pancreatitis. Rev Esp Enferm Dig 103(12):626-631, 2011. PMID: 22217346.
- Kahl S, Glasbrenner B, Leodolter A, et al. EUS in the diagnosis of early chronic pancreatitis: a prospective follow-up study. Gastrointest Endosc 55:507-511, 2002. PMID: 11923762.
- LeBlanc JK, Chen JH, Al-Haddad M, Juan M, Okumu W, McHenry L et al. Endoscopic ultrasound and histology in chronic pancreatitis: how are they associated? Pancreas 43(3):440-444, 2014. PMID: 24622076.
- Noh KW, Pungpapong S, Raimondo M. Role of endosonography in non-malignant pancreatic diseases. World J Gastroenterol 13(2):165-169, 2007. PMID: 17226895.
- Petrone MC, Terracciano F, Perri F, Carrara S, Cavestro GM, Mariani A, et al. Pancreatic abnormalities detected by endoscopic ultrasound (EUS) in patients without clinical signs of pancreatic disease: any difference between standard and Rosemont classification scoring? Pancreatology 14(3):227-230, 2014. PMID: 24854620.
- Pungpapong S, Wallace MB, Woodward TA, et al. Accuracy of endoscopic ultrasonography and magnetic resonance cholangiopancreatography for the diagnosis of chronic pancreatitis: a prospective comparison study. J Clin Gastroenterol 41:88-93, 2007. PMID: 17198070.
- Ripolles T, Martinez MJ, Lopez E, et al. Contrast-enhanced ultrasound in the staging of acute pancreatitis. Eur Radiol 20: 2518-2523, 2010. PMID: 20532782.
- Saftoiu A, Iordache SA, Gheonea DI, et al. Combined contrast-enhanced power Doppler and real-time sonoelastography performed during EUS, used in the differential diagnosis of focal pancreatic masses (with videos). Gastrointest Endosc 72: 739- 747, 2010. PMID: 20674916.
- Timothy B. Gardner, Michael J. Levy. EUS diagnosis of chronic pancreatitis. Gastrointest Endosc 71(5): 1280-1289, 2010. PMID: 20598255.
- Turner BG, Cizinger S, Agarwal D, et al. Diagnosis of pancreatic neoplasia with EUS-FNA: a report of accuracy. Gastrointest Endosc 71:91-98, 2010. PMID: 19846087.
- Uskudar O, Oguz D, Akdogan M, et al. Comparison of endoscopic retrograde cholangiopancreatography, endoscopic ultrasonography, and fecal elastase 1 in chronic pancreatitis and clinical correlation. Pancreas 38:503-506, 2009. PMID: 19287334.
- Varadarajulu S, Eltoum I, Tamhane A, et al. Histopathologic correlates of noncalcific chronic pancreatitis by EUS: a prospective tissue characterization study. Gastrointest Endosc 66:501-509, 2007. PMID: 17640639.
- Varadarajulu S, Tamhane A, Eloubeidi MA. Yield of EUS-guided FNA of pancreatic masses in the presence or the absence of chronic pancreatitis. Gastrointest Endosc 62:728-736, 2005. PMID: 16246688.
- Wiersema MJ, Hawes RH, Lehman GA, Kochman ML, Sherman S, Kopecky KK. Prospective evaluation of endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography in patients with chronic abdominal pain of suspected pancreatic origin. Endoscopy 25(9):555-564, 1993. PMID: 8119204.